Specifying acoustical ceilings for healthcare facilities
By Gary S. Madaras, Ph.D. and Micheal A. Sellitto, M.S., C.I.H.

Healthcare facilities can be complex to design and specify because of unique physical protocols for patient safety, expensive and precise equipment use, and regulatory compliance. The building design can affect productivity, efficiency, economic performance, clinical outcomes, and patient and staff satisfaction. Even experienced healthcare designers and specifiers can have questions about the different building products, assemblies, and systems in healthcare facilities.
Most design aspects of healthcare buildings must satisfy requirements not typical in other building types. For example, ceiling systems in healthcare facilities can have varying acoustical, weight, cleaning, and surface texture requirements that differ by facility type and room function.
This article helps answer common questions healthcare designers and specifiers may have about selecting and specifying ceiling systems. While it focuses on hospitals, outpatient facilities contain many room types with the same requirements as hospitals, minus the inpatient rooms for overnight admittance. Eldercare residential and support facilities, such as nursing homes, are not the focus, but generally, the ceiling requirements in these facilities are more straightforward. One who understands the requirements for hospitals and outpatient facilities should have no difficulty understanding them for residential healthcare and support facilities as well.
Common ceiling requirements
In the United States, the leading set of regulations governing the design and construction of healthcare facilities is the Guidelines1 published by the Facility Guidelines Institute (FGI). All states except four—Illinois, Texas, South Dakota, and Hawaii—have officially adopted and codified FGI’s Guidelines in full or in part or allow them as an alternate compliance path even though they have not officially adopted them.
It is important to understand several common ceiling requirements within the Guidelines for all spaces in hospitals and outpatient facilities. First, “ceilings shall be provided in all areas” (section 2.1-7.2.3.3 in the 2022 version) except for mechanical, electrical, and communications rooms. In these rooms, ceilings are optional. Without ceilings, all the structural members, pipes, conduits, ducts, and wires of the building’s systems would be exposed to the occupied areas below. It would be impractical and ineffective to clean or disinfect all these elements if ceilings were not separating them from the rooms below.
Secondly, ceilings “shall be cleanable with routine housekeeping equipment” (section 2.1-7.2.3.3). Toward this end, ceilings also “shall not create ledges or crevices,” for these could hold dust or debris and not be easily cleaned. Lastly, “all normally occupied hospital and outpatient spaces shall incorporate floor, wall, or ceiling acoustic surfaces” (section 1.2-6.1.3). Since floor and wall surfaces need to be cleaned and disinfected regularly and be able to hold up to considerable wear and impact, the ceilings are the acoustical surfaces typically used to achieve the minimum sound absorption required by the Guidelines.
Healthcare design and specification professionals likely already understand these FGI requirements; rooms must have ceilings free of crevices, be cleanable, and absorb sound. However, the requirements for ceilings do not end there, and this is where some healthcare designers and specifiers start asking questions.
Can any cleanable, crevice-free ceiling be specified for any area?
No, the Guidelines have requirements for ceiling systems and where each can be implemented. Ceiling requirements differ in certain areas because ceiling systems play an essential role in a facility’s ability to maintain asepsis (i.e. cleanliness). As asepsis becomes more important to the function of a given area, ceiling requirements differ.
Three ceiling systems are described in the Guidelines:
- Lay-in ceilings with acoustical ceiling panels (ACPs) with no minimum panel weight requirement and a non-gasketed grid.
- Lay-in ceilings with ACPs that weigh a minimum of
4.88 kg/m² (1 lb/sf) and/or a gasketed grid (at least one; both not required). - Monolithic ceilings.2

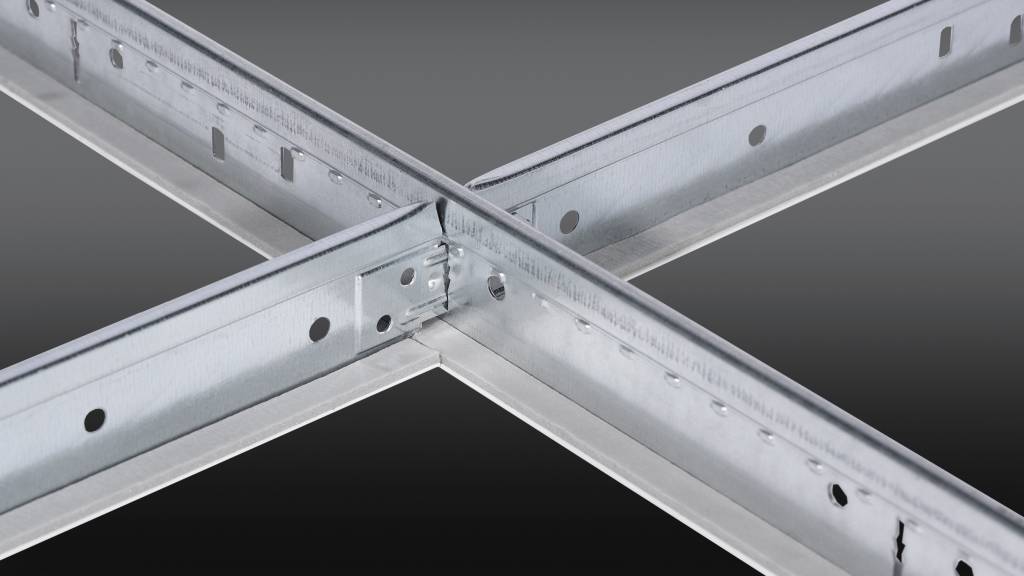
Lay-in ceilings refer to ACPs laid into a standard, metal, tee-bar grid for support, shown in Figure 1, and are acceptable in most healthcare facility areas. For areas that require increased asepsis, where passage of air above the ceiling and the clinical area should be minimized, ACPs need to weigh a minimum of 4.88 kg/m²
(1 lb/sf) and/or a gasketed grid needs to be used, as shown in Figure 2a and 2b on page 10. The Guidelines do not require ceiling panel hold-down clips for any ceiling systems, and ceiling panel clips are not a substitute for the weight minimum or the gasketed grid. For areas where maximum asepsis is required, monolithic ceilings, such as painted gypsum board, must be implemented and are defined as free of fissures, cracks, and crevices.

What is different about specific areas that require special ceiling features?
Broadly explained, the ceiling specification required by the Guidelines is determined by the types of procedures for which the space is designed.3
In most areas of healthcare facilities, invasive procedures are not performed on patients. This includes rooms for medical purposes, such as examination rooms, laboratories, and most emergency department spaces. ACPs have no minimum weight requirement, and a non-gasketed grid is permitted. In addition, all areas for nonmedical uses, such as administrative areas, public areas, waiting rooms, and eating spaces, permit ACPs with no minimum weight and a non-gasketed grid.
Where minimally invasive surgical, diagnostic, and therapeutic procedures are performed, as well as areas serving operating rooms, the Guidelines permit lay-in ceilings with ACPs that weigh a minimum of 4.88 kg/m² (1 lb/sf) and/or a gasketed grid. Some examples are Class 2 imaging rooms, endoscopy and bronchoscopy rooms, neonatal intensive care, clean/sterile corridors, operating room equipment storage rooms, and sterile processing rooms. In addition, most laundry areas have these requirements.

To reduce the chance of infection, rooms for surgically invasive procedures requiring an aseptic surgical field, such as operating rooms (Figure 3) and Class 1 imaging rooms, must have monolithic ceilings. Standard lay-in ceilings are not permitted. In addition, areas for immunocompromised patients, such as bone marrow transplant, burn, and oncology areas, including associated toilet rooms, also fall under these requirements. Most areas for behavioral health patients also require monolithic ceilings to meet ligature-resistant requirements.
What are the differences in the requirements for unrestricted, semi-restricted, and restricted areas?
Designating a space as unrestricted, semi-restricted, or restricted can be a good starting point for determining which types of ceiling systems are permitted in that area.

Unrestricted areas (Figure 4) include most areas of healthcare facilities outside of operating rooms (and other rooms in which surgical or other invasive procedures are performed) and their peripheral support spaces. Where ceilings are required, ACPs are mostly permitted without the panel weight or gasket requirements. Exceptions to these ceiling requirements in unrestricted areas are discussed later in this article.

Semi-restricted areas are intended to separate unrestricted and restricted areas and include peripheral support areas for restricted areas, such as endoscope processing rooms, decontamination rooms, clean corridors (Figure 5), and central sterile supply. Where ACPs are implemented in semi-restricted areas, they must weigh a minimum of 4.88 kg/m² (1 lb/sf) and/or have a gasketed grid. Ceilings of this type are also required in other areas.
Restricted areas can only be accessed through semi-restricted areas; access is restricted to maintain asepsis rather than security and usually has garbing requirements. These include operating rooms, Class 3 imaging rooms, and protected environment rooms. Ceilings in restricted areas must be of monolithic construction, meaning ACPs are not allowed in these areas. Alternatives in the 2022 Guidelines are clarified later in this article. Monolithic ceilings are required in other areas as well.
Are there any exceptions to know regarding these general requirements?
Yes, there are quite a few exceptions to these general requirements, most of which apply to unrestricted areas. Some examples, all of which are unrestricted areas, are mechanical spaces, which do not require ceilings (though they are permitted); public corridors require ceilings, but ACPs have no weight or gasketed grid requirement; airborne infection isolation (A.I.I.) rooms require ceilings with a weight minimum of 4.88 kg/m² (1 lb/sf) and/or a gasketed grid; behavioral health areas require monolithic ceilings.
Other notable exceptions may be in hospitals’ laundry areas, food preparation areas, food supply, and storage rooms. In these spaces, if lay-in ceilings are implemented, the ACPs must weigh a minimum of 4.88 kg/m² (1 lb/sf), and a gasketed grid alone does not meet this requirement. Note that this does not apply to those areas in outpatient or residential facilities, where lay-in ceilings with ACPs with no weight minimum and a non-gasketed grid can be implemented in all laundry, food preparation, supply, and storage areas.
Additionally, the 2022 Guidelines allow for alternative, prefabricated ceiling systems4 in operating rooms, cesarian delivery rooms, and Class 3 imaging rooms that are not monolithic. Refer to section 2.1-7.2.3.3(3).
How does one determine which type of ceiling system should be specified for any area?
This article goes a long way toward informing specifiers about ceiling requirements in healthcare facilities. However, since some exceptions and nuances exist, one should refer to an online, easy-to-follow reference document. It details ceiling requirements by healthcare facility type, department, and room function.5
FGI outlines much of the rationale for ceiling requirements in healthcare facilities in a 2022 publication called “Applying the FGI Guidelines to Spaces Where Invasive vs. Noninvasive Patient Care is Delivered” on its website.4 The Guidelines also include tables to understand ceiling requirements in some rooms, though they are not nearly as comprehensive as the previously cited online resource.
In general, monolithic ceilings are required in restricted areas and other areas requiring maximum asepsis, such as those for immunocompromised patients, such as burn and oncology patients, those with certain airborne infections, toilet rooms that service those patients, as well as pharmacy clean rooms, and Class 3 imaging rooms. All behavioral health patient areas require monolithic ceilings. ACPs are not permitted.
ACPs with a minimum weight of 4.88 kg/m² (1 lb/sf) and/or a gasketed grid are required in semi-restricted areas and some invasive procedure and diagnostic areas, such as cardiac catheterization, trauma rooms, A.I.I. and their associated anterooms, some procedure rooms, Class 2 images rooms,
and others.
ACPs with no other requirements are allowed in most, but not all other areas, including public areas such as waiting areas, corridors, lobbies, reception, dining, shops, and toilet rooms, as well as staff and administrative areas, such as offices, lounges, conference rooms, and sleeping quarters. In addition, these requirements apply to all non-surgically invasive patient areas, such as patient rooms and patient toilet rooms, laboratories, Class 1 imaging rooms, dialysis, nuclear medicine, labor, delivery, recovery, and postpartum, just as examples.
Do eldercare residential facilities differ significantly from these FGI ceiling requirements?
These health facilities include nursing homes and hospices, residential care, and support facilities, such as assisted living, independent living, and long-term residential substance use disorder treatment facilities, and nonresidential support facilities, such as adult day care, wellness centers, and outpatient rehabilitation therapy facilities. Invasive medical procedures are not typically performed in most rooms in these facilities. Therefore, neither ceiling panels with a minimum weight of 4.88 kg/m² (1 lb/sf) nor specialty gasketed grids are required.
However, one exception could be A.I.I. rooms, including their associated ante-rooms, if they occur in the project. In healthcare facilities such as nursing homes and hospices, A.I.I. rooms require either a gasketed grid or ceiling panel with a minimum weight of 4.88 kg/m² (1 lb/sf). In behavioral health departments or facilities, all patient areas are required to have a monolithic ceiling. ACP ceilings are not permitted.
How do acoustical requirements factor into the ceiling specifications?
Beyond the previously mentioned requirement that all normally occupied spaces shall incorporate floor, wall, or ceiling acoustical surfaces, tables 1.2-3 in the Outpatient and Residential Guidelines and table 1.2-4 in the Hospitals Guideline further define the minimum design room-average sound absorption coefficients for different types of rooms.
This acoustical metric, unique to FGI’s Guidelines, is an area-weighted average of the Noise Reduction Coefficient (NRC) ratings of the floor, walls, and ceiling. Values range from 0.10 to 0.25, but 0.15 and 0.20 apply to most patient care and clinical spaces. Absorption requirements drop to 0.10 in large common spaces such as atriums, dining spaces, and natatoriums. They increase to 0.25 in telemedicine and waiting rooms close to patient care areas.
To better understand FGI’s absorption metric, consider an example. A patient room in a hospital is required to have an absorption coefficient no lower than 0.15. It would comply if the floor had an NRC of 0.15, the walls had an NRC of 0.15, and the ceiling had an NRC of 0.15—but this is all unlikely. The floor is probably a hard, nonporous, and sound-reflective material, such as sheet vinyl, so it is easier to clean and durable. This means the other room surfaces need to be more sound absorptive. For example, the walls and ceiling might need NRC ratings of 0.55. The walls will most likely be a hard, nonporous, and sound-reflective material, such as painted gypsum board. This means the ceiling NRC rating needs to be even higher, perhaps as high as 0.80 or 0.90, to provide a room-average coefficient of 0.15. The exact NRC ceiling rating can vary greatly and depends on the room size and proportions. The formula below yields the required ceiling NRC when the floor and walls are sound-reflective.
NRCC = CFGI * AT AC
Where:
NRCC—The NRC rating of the ceiling that should be specified
CFGI—The coefficient required by FGI from tables 1.2-3 or 1.2-4 (most frequently 0.15 or 0.20, but could be as high as 0.25 or as low as 0.10)
AT—The total area of all room surfaces
(AreaCeiling + AreaFloor + AreaWalls)
AC—The total area of the ceiling (length x width)
Do the ceiling acoustical requirements in the Guidelines align with those in HIPAA and EBD?
Unfortunately, the three are unrelated, and understanding each can be important.
According to the Center for Health Design, evidence-based design (EBD) is basing decisions about the built environment on credible research to achieve the best possible outcomes. A growing body of evidence attests that the physical environment impacts patient stress, patient and staff safety, staff effectiveness, and the quality of care provided in hospitals and other healthcare settings.
There is a strong acoustics component to EBD. Design interventions impacting safety, quality, and cost include using high-performance, sound-absorbing ceiling panels. Specifying and using high NRC ceiling panels of 0.90 or more has been proven to reduce patient and staff stress and patient sleep deprivation and increase patient satisfaction.7
The Health Insurance Portability and Accountability Act (HIPAA) of 1996 protects the privacy and security of health information regardless of whether it is written, digital, or spoken. HIPAA’s Privacy Rule includes oral exchange of information. It generically requires reasonable efforts to maintain privacy and security during spoken conversations, whether in person or over communication devices. However, HIPAA has no ceiling requirements. If one were asked to support those reasonable efforts made during the design and specification of a healthcare facility to ensure speech privacy, pointing to a specification of a high NRC ACP ceiling would suffice and be consistent with EBD. However, a specification for a sound-reflective ceiling would not be sufficient.
EBD is best practice but optional from a federal or state governmental perspective. It shows the positive impact specifying high NRC ceilings has on safety, quality, and cost. Most states have codified the FGI Guidelines, and therefore, compliance is required in those states. FGI’s acoustical requirements for ceilings vary greatly and require calculations based on room dimensions and finishes used on the floor, walls, and ceiling. HIPAA is a federal act; compliance is mandatory in every facility where health information is exchanged. However, there are no requirements defined for ceilings.
Conclusion
Specifying ceiling systems for healthcare facilities does not need to be daunting if one understands the few overarching FGI requirements, follows the general guidance in this article, and then double-checks for exceptions using the referenced online resources.
- Ensure a contiguous ceiling free from ledges and crevices that could hold dust and be cleaned with routine housekeeping equipment is specified.
- Use the formula in this article and the rooms’ dimensions to specify the appropriate minimum ceiling NRC rating. To avoid numerous lay-in panel types in the specification, one might need to default to the highest NRC for all the ceilings or, perhaps, a mid-NRC ceiling panel and a high-NRC panel.
- In most spaces in healthcare facilities, such as public, administrative, and clinical areas where invasive procedures are not performed, no ceiling requirements other than those above must be specified. This provides design freedom in materials, colors, textures, and patterns for improved aesthetics.
- Semi-restricted spaces exist between unrestricted and restricted areas. In these areas, as well as some invasive procedures and diagnostic areas, the grid must be gasketed, and/or lay-in ceiling panels must weigh a minimum of
4.88 kg/m² (1 lb/sf). - A small number of spaces where invasive medical procedures are performed can be classified as restricted. Here and in other areas with immunocompromised or behavioral health patients’ ceilings need to be monolithic. Lay-in ACPs are not permitted.
- Lastly, check the list of exceptions in the online resources and this article.
Notes
1 Refer to the Facility Guidelines Institute’s (FGI’s) Guidelines online at https://fgiguidelines.org/guidelines/editions/.
2 In Class 3 Imaging Rooms, Operating Rooms (Class B and C), and Surgical Cystoscopic Rooms where monolithic ceilings are required in the 2018 FGI version, the 2022 FGI version allows monolithic ceilings or other alternative, prefabricated ceiling systems per section 2.1-7.2.3.3(3).
3 See FGI 2022. “Applying the FGI Guidelines to Spaces Where Invasive vs. Noninvasive Patient Care is Delivered” at https://fgiguidelines.org/
wp-content/uploads/2023 /09/Application-Guidance invasive-1.pdf.
4 The FGI’s appendix language A2.1-7.2.3.3 (3)(b) describes one example, laminar flow ceilings.
5 Refer to The Environmental Health and Engineering, Inc. document, available online at https://www.rockfon.com/syssiteassets/rockfon-na/downloads/fgi-acoustic-ceiling-panels-requirements-for-health-care-facilities.pdf.
6 For more, review tables 2.1-4 and 2.1-5 in FGI’s Outpatient Guidelines and tables 2.2-1 and 2.2-2 in the Hospitals Guidelines.
7 Review the Center for Health Design whitepaper, “The Business Case for Building Better Hospitals Through Evidence-Based Design at www.healthdesign.org/chd/research/business-case-building-better-hospitals-through-evience-based-design.
Authors

Gary Madaras, Ph.D., is an acoustics specialist at Rockfon, an acoustical ceiling solutions manufacturer. He helps designers and specifiers learn the optimized acoustics design approach and apply it correctly to their projects. He is a member of the Acoustical Society of America (ASA), the Canadian Acoustical Association (CAA), and the Institute of Noise Control Engineering (INCE). Madaras can be reached at gary.madaras@rockfon.com.

Michael Sellitto, M.S., C.I.H., is an industrial hygienist at Environmental Health & Engineering. He conducts research in occupational settings, including healthcare, manufacturing, and life sciences, and is experienced in exposure assessments, exposure modeling, and indoor air quality. He is a member of the American Industrial Hygiene Association (AIHA). He can be reached at msellitto@eheinc.com.
Key Takeaways
Healthcare facility ceiling design is guided by Facility Guidelines Institute (FGI) standards, prioritizing patient safety, asepsis, and acoustical requirements. Ceilings must be cleanable, free from crevices, and acoustically absorbent. Most spaces, such as public and administrative areas, allow for design flexibility with lay-in acoustical panels. However, semi-restricted spaces require heavier panels or gasketed grids, and restricted areas, including operating rooms, mandate monolithic ceilings for maximum asepsis. Acoustical panels enhance sound absorption, supporting privacy and comfort in patient areas. Healthcare designers should consult FGI Guidelines to ensure compliance and adapt specifications for specific room types and unique requirements.
Sign up for our weekly newsletter
Architectural materials and methods delivered right to your inbox
- CSI News and Notes: CSI Foundation’s construction camp; CSI spring exam; and more
- CSI News and Notes: CSI’s credentials; CSI conference theme; and more
- To be specific – CSI supports young AECO professionals
- CSI News and Notes: CSI’s foundation scholarships, national conference, and Crosswalk
- CSI News and Notes: AI’s impact; CSI 2024 conference, and more


Read the Latest Issue