Where Performance Drives Specifications: Medical office buildings and enclosure system selection
by Katie Daniel | December 12, 2016 10:14 am

by Paul Brown
Specification writers must now consider more performance criteria than ever before. As trends in sustainability and wellness evolve and gain traction with building owners, and as the list of new products continues to grow, design professionals must determine how to reach more stringent targets for indoor environmental quality and energy consumption.
For any specifier tasked with improving performance above standard construction outcomes, simplicity should be the guiding mantra. For instance, those specifications that rely on precision installation from multiple parties rarely work well, due to the shared accountability inherent in complex systems. Taking a more simplified global look at performance targets can yield an enlightened focus on the enclosure system—one that can help a project meet higher standards.
Medical office facilities often fall prey to the destructive combination of higher performance criteria and a tendency to overcomplicate specifications. Historically, many owners have not viewed their buildings as necessary components to providing care. In fact, most have invested heavily in people and equipment rather than the building itself. However, owners are now becoming increasingly aware of the building and indoor environment’s critical role in enhancing standards of care and levels of healing.
A study from the Lawrence Berkeley National Lab (LBNL), “Health and Productivity Gains from Better Indoor Environments and Their Relationship with Building Energy Efficiency,” concludes that improvements to indoor environments can reduce the transmission of respiratory diseases by nine to 20 percent. (William J. Fisk’s study, “Health and Productivity Gains from Better Indoor Environments and Their Relationship with Building Energy Efficiency,” was published by Lawrence Berkeley National Lab in 2000.) This in turn can reduce absenteeism and increase cognitive function of doctors, nurses, and caregivers. Another study, by Johns Hopkins University, directly links patient care to the acoustic quality of a space. (Details on John Hopkins University’s piece, “Rise in Hospital Noise Poses Problems for Patients and Staff,” can be found at www.sciencedaily.com/releases/2005/11/051121101949.htm[1].) Poor indoor air quality (IAQ), inadequate thermal control, and lack of acoustic privacy all impede quality of care—problematic not only for caregivers and patients, but also for business success.
Medical facilities are generally among the most expensive building types to operate and maintain. The U.S. Department of Energy’s (DOE’s) analysis of data from the last five years indicates medical office buildings have a median source energy use intensity (EUI) of 245 kBtus/sf, with some exceeding 570 kBtus/sf. This is significantly higher than data collected through the Commercial Buildings Energy Consumption Survey (CBECS) in 2012, which indicated a median EUI of 194 kBtus/sf. (The U.S. Department of Energy published “Energy Use in Medical Office Buildings, Portfolio Manager,” in January 2015.)
As indoor medical environmental standards have tightened, retrofits on older buildings have begun to make less financial sense, given the basic elements of the enclosure were never constructed to address high-performance standards. Such poor enclosures cause energy use and operational expenses to skyrocket, as HVAC systems must work hard to maintain the environmental standards required in medical facilities.
Owners need not only newer facilities that can reduce utility costs, but also spaces that help improve the standard of care for medical staff and their patients. Energy-efficient buildings featuring top-class IAQ, acoustic privacy, and thermal comfort are all necessary for owners’ financial success.
Tighter enclosure standards
One challenge this new demand for high-performance buildings presents specifiers is the difficulty of updating older buildings. That is, it is challenging to turn buildings that were constructed under entirely different standard specifications into the high-performance buildings of today. If the basic components of the building are incompatible, little can be done.
For example, wall construction and several other components of the building’s enclosure are the first line of defense for any high-performance building. If these are incorrectly installed, no mechanical system can fix the resulting issues. When done properly, however, mechanical systems can be downsized, have a longer lifespan, and operate efficiently, all while achieving higher IAQ standards.
Simply meeting code compliance for various building envelope components will not provide the benefits now sought by medical office building owners. The following sections highlight performance recommendations for building enclosures based on the aforementioned studies and the business imperatives of medical office building owners.

Indoor air quality
Top-tier air quality is needed for the effective care of patients in any medical office building. Providing a space that is clear of mold, mildew, volatile organic compounds (VOCs), and particulates is critical to the success of a facility. Filters included in mechanical equipment, if they are not combined with proper sealing of the building envelope, may not prevent uncontrolled air from entering a facility. A study conducted by the American Society of Heating, Refrigerating, and Air-conditioning Engineers (ASHRAE) indicates air infiltration rates in standard construction can be as many as five to seven air changes per hour (ach). This study also suggests that less than 1 ach is achievable if the wall is specified and constructed carefully. (This information comes from “Setting Air Tightness Standards,” a piece completed for the ASHRAE Journal, [vol. 47, no. 9], in September 2005.)
Thermal comfort
Patients undergoing treatment and examinations are sensitive to changes in air speed, wide bands of air temperatures, and dissimilar radiant surfaces between interior and exterior walls. In medical facilities, even modest changes in the thermal environment can create exaggerated sensations that dramatically affect patients’ mindsets and providers’ ability to support them. As such, the thermal ‘comfort zone’ for medical office buildings is generally tighter than ASHRAE 55, Thermal Environmental Conditions for Human Occupancy. A dead-band of only one to two degrees of air temperature, air speeds less than 190 cfm, and radiant temperature equal to room temperature is also suggested. (The Journal of Hygiene published R.M. Smith and A. Rae’s study, “Thermal Comfort of Patients in Hospital Ward Areas,” in 1977.)
Acoustics
Medical environments have steadily increased in volume as sirens, alarms, and urban locations have gained traction. These higher levels of background noise not only impede communication between care providers and patients, but also increase levels of stress. This can affect decision-making by care providers as well as a patient’s ability to cope and heal. To mitigate sound transmission, the enclosure should target a sound transmission class (STC) greater than 55—a number that, according to the Ceilings & Interior Systems Construction Association (CISCA), has proven to be the sweet spot needed for acoustic well-being. (The Ceilings & Interior Systems Construction Association released this information in a report, “Acoustics in Healthcare Environments” in October 2010.)
Energy performance
The effective R-value of the building envelope dictates the amount of energy required to produce and maintain performance. However, most calculations for energy performance fail to fully account for the effects of thermal bridging. Thermal bridging occurs when heat gain or loss is more quickly transferred through wood or metal studs in a lightweight building assembly (LBA), or directly through a mass wall constructed of tilt-up concrete or concrete masonry units (CMUs). To compensate for this, HVAC designers often over-size systems to ensure there is enough capacity to meet thermal comfort—a strategy which in turn leads to reliance on equipment that runs less efficiently than equipment that is properly sized.
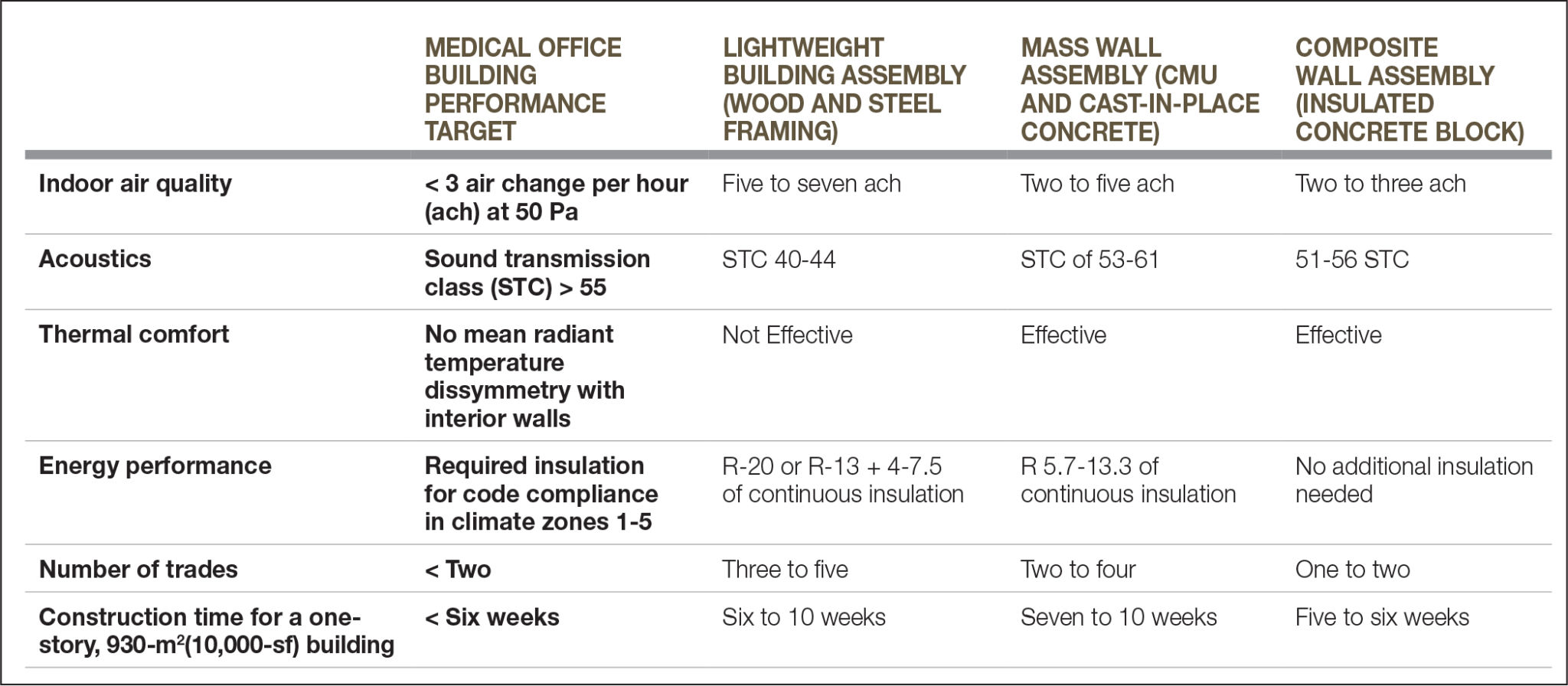
Selecting the right enclosure system
Three categories of wall enclosures are generally used in medical office buildings:
- LBAs such as wood and steel framing;
- mass wall assemblies such as concrete masonry units (CMUs) and concrete; and
- composite wall assemblies that combine multiple materials (such as insulated concrete block).
When high air quality, acoustics, and thermal control performance standards are applied, the initial cost of wall materials is no longer the best factor to consider when determining what is best for a project. Materials that were historically hidden behind interior and exterior finishes have become the most important considerations a specifier can make. The performance of each of the wall components, and how they interact with each other, determines whether an enclosure can achieve the performance criteria listed above.
Lightweight building assemblies
Wood and steel stud cavity wall construction have historically been selected due to their low cost and easy construction. These materials are simple to find and price, and trades have been using them for years. However, once performance criteria for air, acoustics, thermal, and energy performance are considered, such LBAs rapidly become the most complex system to specify.
The challenge with lightweight framing is the number of parts to the system. Studs, sheathing, cavity insulation, continuous insulation, air/water barriers, interior finishes, and exterior finish materials all play a part in the overall performance of the system. A single poorly selected component, such as interior wallcoverings that inadvertently trap moisture in the wall, can impede the performance of the other components of the system.
Inexperienced or unskilled subcontractors can cause the same issues as badly specified components; one poorly installed material can render all the properly installed components ineffective. With the advent of field testing and envelope commissioning services to verify performance target achievement, contractors often find themselves at the center of a complex debate when test failures occur. Many parties scramble to assign fault if this happens—and must also find solutions to fix the installation after it is complete. Thus, trades that have historically functioned independently must now work together to achieve a high-performing enclosure.
Together, various medical office building performance criteria can increase the complexity of light frame construction. Speed, flexibility of parts, and the low level of skill needed for installation may all be benefits of LBAs, but all these benefits interfere with the tight, integrated, and coordinated construction necessary to fit performance criteria.

Mass wall assemblies
Mass wall assemblies—mainly CMU and tilt-up concrete panel construction—are appealing to medical office building owners and specifiers because they simplify wall construction. The fluid-applied vapor barriers used on mass walls perform better than the sheet-applied vapor barriers used on LBAs, due to the fact that the wall is more rigid. This can lead to reduced air infiltration and improved IAQ. The mass of wall also eliminates dissimilar radiant temperature differences between interior and exterior surfaces, thereby increasing thermal comfort. Finally, the mass reduces transmission of noise from outside to inside, improving privacy and ease of communication for patients and their caregivers.
Still, many of the challenges that occur with LBAs are also present in mass wall assemblies. Often, a second wall of metal studs is installed over continuous insulation to provide an attachment point for interior or exterior finishes. This second wall is not needed for overall performance, but nonetheless adds an extra step that increases construction and coordination time. The overall construction schedule and sequence is significantly affected.
Mass wall assemblies are considered the baseline enclosure system for medical office buildings, as they exhibit the qualities required for air, acoustics, thermal, and energy performance. This enclosure system is solid, performing well thermally and acoustically, and there is less chance one trade will impact the performance of the wall. However, this assembly takes more time to construct and is more expensive than LBAs. That being said, as owners look beyond initial costs, its long-term benefits overcome these drawbacks, making it suitable for use as a baseline system.
Composite wall assemblies
Despite mass wall assemblies’ advantage over LBAs, the fact remains these systems were never designed to meet the requirements for high-performance building envelopes. They both fail to take advantage of the potential that comes with designing a system specifically to address air, acoustic, thermal, and energy performance from the outset—unlike the newer composite materials beginning to gain traction.
A relatively new entry to this market is the insulated concrete block. It is specifically designed to address the main weaknesses found within both LBAs and mass wall systems, such as the inherent complexity that comes with multiple layers of materials installed by multiple trades.
An insulated concrete block integrates continuous insulation within the masonry unit. Once in the field, one trade is required to install the system, with only one other needed to apply the air/vapor barrier. Once filled with concrete, the wall system is considered complete, and the addition of finish materials to the inside or outside of the wall have little to no impact on its overall performance.
With these characteristics (minimal trade involvement and material requirements, along with effective insulation), all the performance criteria of medical office buildings can be achieved. By specifying insulated concrete block, specifiers can remove most of the barriers inherent to specifying walls for high-performance envelopes. Walls of these materials can be constructed more quickly, with fewer trades to coordinate, and often at a lower cost than more traditional assemblies. Further, they can perform better.
Insulated concrete block has been predominantly used in the South, Southwest, and Pacific West portions of the United States, but is ideal for use in many other parts of the country. It meets 2015 International Energy Conservation Code (IECC) requirements for wall insulation in climate zones one through five, including areas containing a significant majority of the U.S. population. Insulated concrete block also provides significant windstorm protection for projects located in hurricane- and tornado-prone areas, which includes the central plains, Gulf Coast, and East Coast of the United States. Projects in all areas can benefit from the fire safety, healthiness, and comfort provided by insulated concrete block.
Only extreme temperatures affect the installation of this material, as with all other types of concrete construction. The stacking of the block is limited to the foam adhesive application temperature limits (-4 to 49 C [25 to 120 F]), and the concrete pour is limited by American Concrete Institute (ACI) standards for especially hot or cold days.
The biggest challenge to widespread adoption of insulated concrete block and other composite materials is the change required from those who design, specify, and construct buildings. Construction is a system whose commodity pricing relies on people who are more willing to take on financial risk if they can control the outcome. Education, experience, and expertise are needed throughout the specification and bidding process to ensure composite materials can be adopted by the contractor.
By understanding the simplicity that comes with composite materials, specification writers can help owners, designers, and contractors understand how this solution—new or otherwise—can be the best way to achieve mutual success.
Beyond medical office buildings
Owners of medical office buildings may well be at a tipping point for increased performance criteria. These buildings’ unique purpose—the care and nurturing of human life—prompts owners to lay the groundwork for healthy, productive, and energy-efficient building construction standards.
However, other building types can likewise realize the potential of exploring a more simplified building product. Offices, retail buildings, assemblies, and public facilities can also benefit from spaces that address air, acoustics, thermal, and energy performance criteria. Specification writers who understand the demand for performance, the performance criteria that meet that demand, and how composite materials can be used to control building outcomes will be poised to ride the wave of sustainable and healthy buildings for years to come.
Paul Brown, MBA, LEED GA, is president of Bautex Systems[2], a manufacturer of insulated concrete block for building envelope and other wall systems. He writes about design and construction of mass wall systems to meet new energy and life safety codes for commercial and residential buildings. Brown is also a board member at-large for the U.S. Green Building Council (USGBC), Texas chapter. He can be contacted via e-mail at paul.brown@bautexsystems.com[3].
- www.sciencedaily.com/releases/2005/11/051121101949.htm: http://www.sciencedaily.com/releases/2005/11/051121101949.htm
- Bautex Systems: http://www.bautexsystems.com
- paul.brown@bautexsystems.com: mailto:paul.brown@bautexsystems.com
Source URL: https://www.constructionspecifier.com/where-performance-drives-specifications-medical-office-buildings-and-enclosure-system-selection/